Health Clinical Research article published by Dr. Pazhaniyappan BSMS
Gallbladder diseases have become increasingly common worldwide, often causing severe abdominal pain and life-threatening complications when untreated. Conditions such as cholecystitis, acute pancreatitis, and obstructive jaundice frequently occur together due to gallstone-related blockage in the bile ducts.
A recent clinical case study from Rathna Siddha & Herbal Research Centre in Chennai suggests that traditional Siddha-based therapeutic intervention may help manage these acute hepatobiliary disorders without surgical procedures in selected cases.
The study documents the recovery of a 29-year-old female patient who presented with acute abdominal pain, nausea, vomiting, loss of appetite, and disturbed sleep. Clinical evaluation and laboratory investigations revealed significantly elevated liver enzymes and bilirubin levels, indicating serious hepatobiliary inflammation.
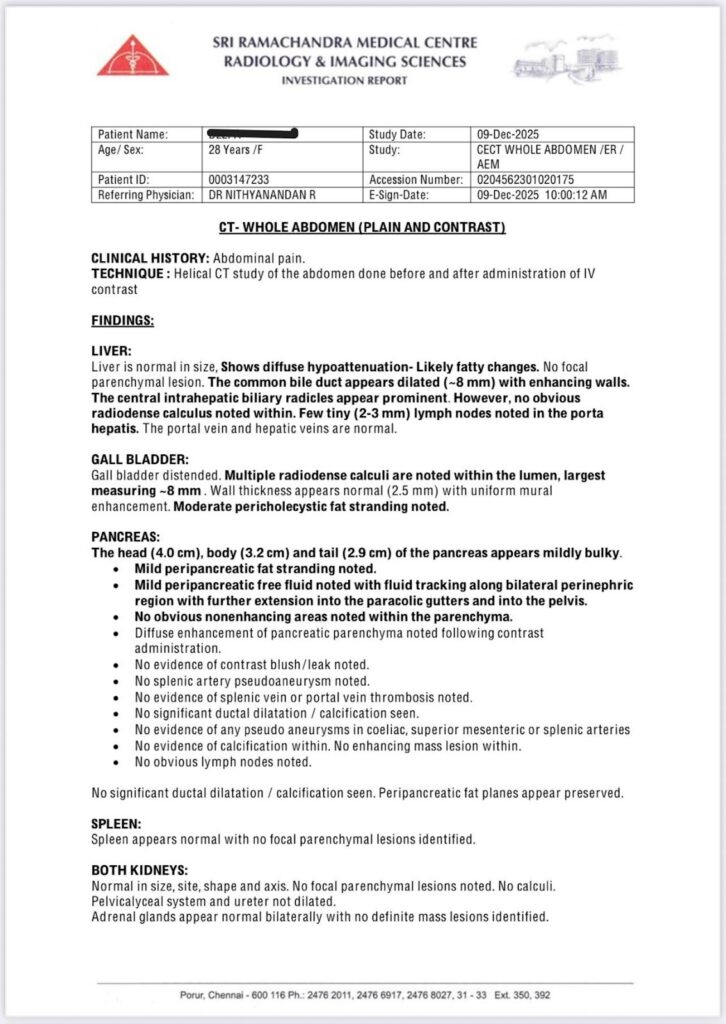
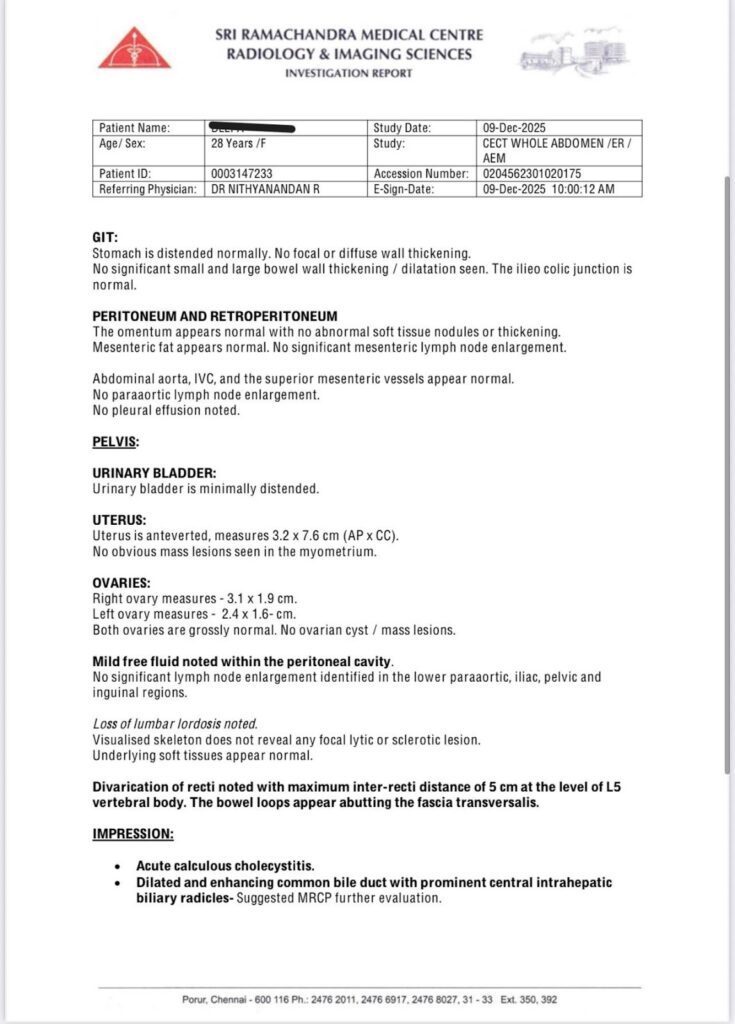
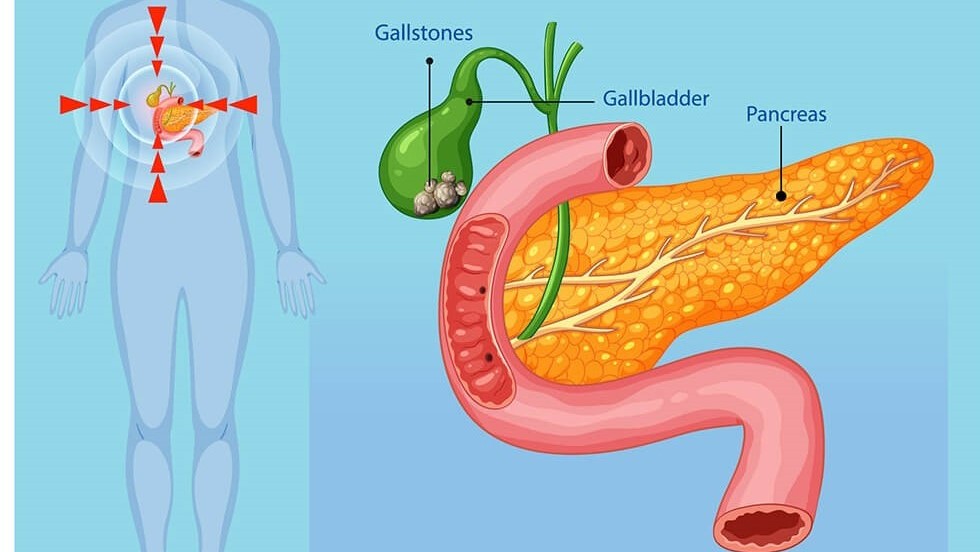
Ultrasound and radiological examinations confirmed the presence of acute calculous cholecystitis, dilation of the common bile duct suggesting biliary obstruction, and early signs of acute pancreatitis likely triggered by gallstone migration.
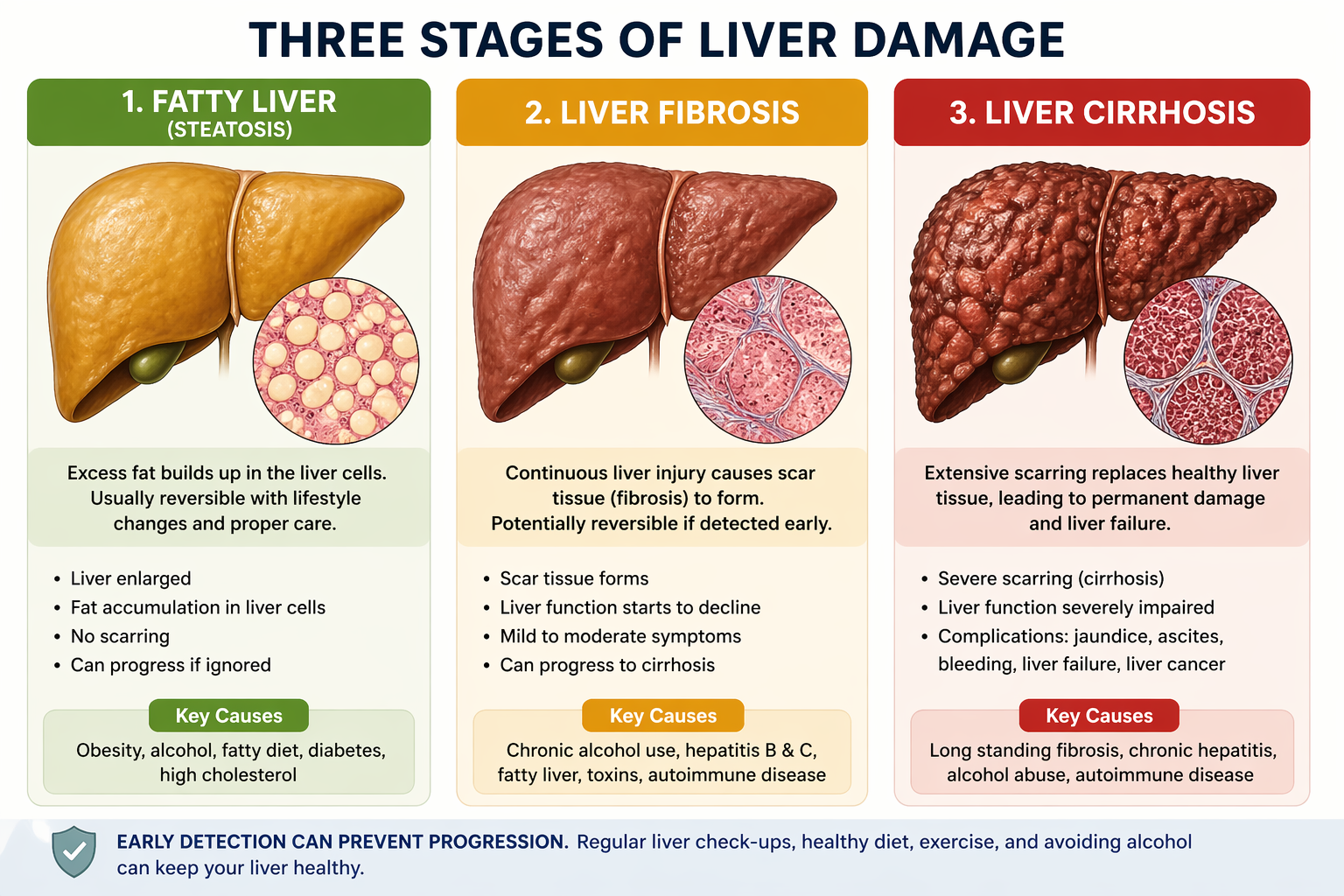
According to modern medical understanding, cholecystitis occurs when gallstones block the cystic duct, causing bile accumulation and inflammation of the gallbladder wall. This obstruction can also disrupt pancreatic drainage, leading to pancreatic inflammation and jaundice due to elevated bilirubin levels in the blood.
Because of the risk of complications, contemporary medical practice often recommends surgical or interventional procedures to relieve obstruction and control inflammation.
However, in this reported case, the patient was admitted for integrative Siddha-based inpatient management rather than immediate surgery. The treatment included herbal formulations, therapeutic juices, dietary regulation, and continuous monitoring of vital parameters and biochemical markers.
Within three days of therapy, the patient experienced significant relief from symptoms such as fever, abdominal pain, vomiting, and reddish discoloration of urine. Jaundice symptoms gradually subsided as treatment progressed.
Laboratory investigations showed a remarkable improvement in inflammatory and hepatic parameters.
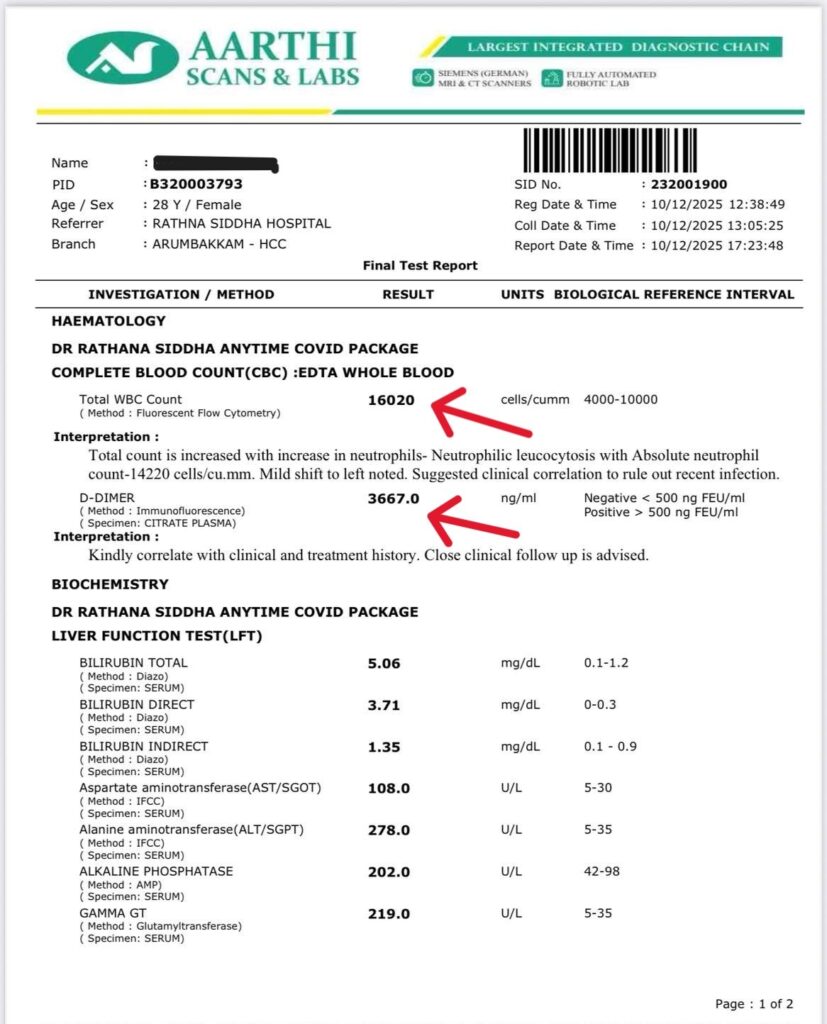
Before treatment, the patient exhibited marked leukocytosis, with a white blood cell count of 16,020 cells/cumm and elevated D-dimer levels indicating systemic inflammatory activity. Liver function tests showed severe biochemical disturbance, including total bilirubin levels of 5.06 mg/dL, ALT of 278 U/L, AST of 108 U/L, and elevated alkaline phosphatase and GGT levels.
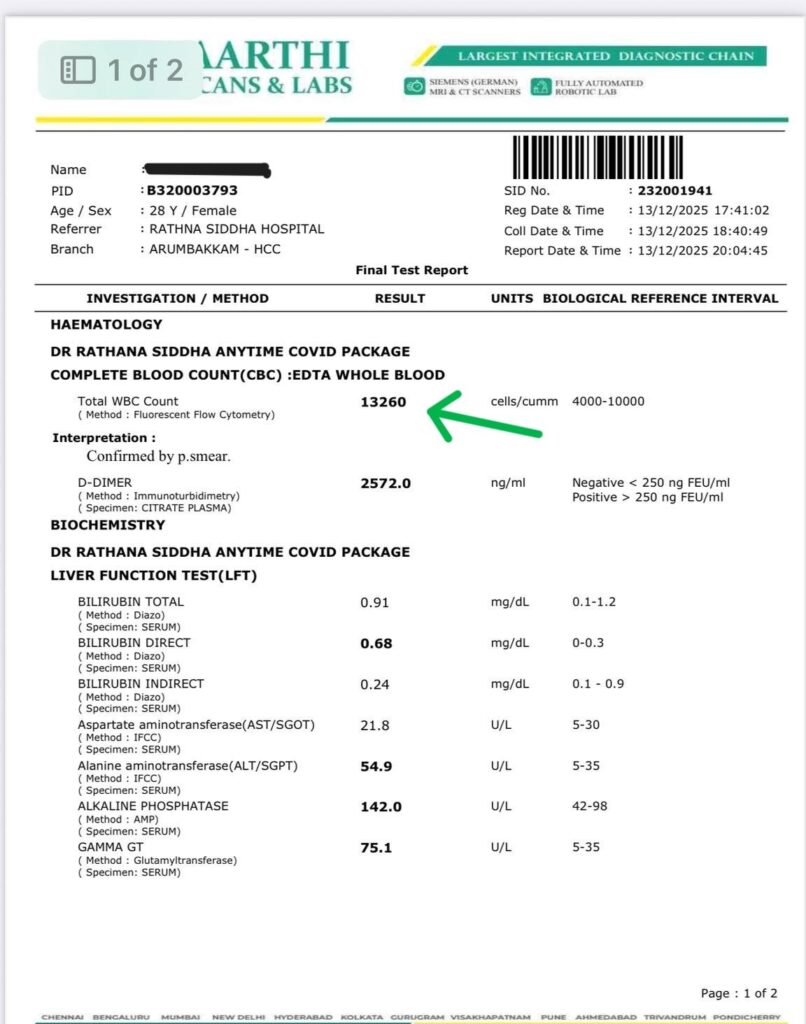
Following the Siddha therapeutic regimen, follow-up investigations revealed significant normalization of these values. Total bilirubin decreased to 0.91 mg/dL, ALT reduced to 54.9 U/L, AST dropped to 21.8 U/L, and GGT levels declined substantially. These changes corresponded with the patient’s clinical recovery and disappearance of jaundice.
Researchers observed that the patient tolerated the treatment well, with no adverse effects reported during hospitalization or follow-up. The reduction in inflammatory markers and restoration of liver enzyme levels suggested effective resolution of hepatobiliary inflammation.
The findings highlight the potential role of Siddha and traditional medicine–based treatment approaches in modulating inflammatory responses, supporting liver function, and promoting recovery in certain acute hepatobiliary conditions.
While this report represents a single clinical case, the results indicate that traditional therapeutic systems may offer supportive strategies for managing complex disorders involving the gallbladder, liver, and pancreas.
| Parameter | Before Treatment10/12/2025 | After Treatment13/12/2025 | Reference Range | Objective Interpretation |
| Total WBC Count (cells/cumm) | 16,020 | 13,260 | 4,000–10,000 | Significant reduction in inflammatory response |
| Absolute Neutrophil Count (cells/cumm) | 14,220 | Not specified | 1,500–7,500 | Resolution trend of neutrophilic leukocytosis |
| D-Dimer (ng/ml) | 3,667 | 2,572 | < 250–500 | Marked reduction in systemic inflammatory–coagulatory activity |
| Total Bilirubin (mg/dL) | 5.06 | 0.91 | 0.1–1.2 | Normalization of bilirubin metabolism |
| Direct Bilirubin (mg/dL) | 3.71 | 0.68 | 0–0.3 | Significant improvement in cholestasis |
| Indirect Bilirubin (mg/dL) | 1.35 | 0.24 | 0.1–0.9 | Return toward physiological range |
| AST / SGOT (U/L) | 108.0 | 21.8 | 5–30 | Resolution of hepatocellular injury |
| ALT / SGPT (U/L) | 278.0 | 54.9 | 5–35 | Marked reduction in hepatic inflammation |
| Alkaline Phosphatase (U/L) | 202.0 | 142.0 | 42–98 | Improving biliary obstruction |
| Gamma GT (U/L) | 219.0 | 75.1 | 5–35 | Significant reduction in biliary enzyme elevation |
Further research with larger clinical studies will be necessary to better understand the mechanisms and therapeutic potential of Siddha interventions in hepatobiliary and pancreatic diseases.
The study was published by Rathna Siddha & Herbal Research Centre, Chennai, Tamil Nadu, India.