Research Article
Dr.Pazhaniyappan BSMS
published by Rathana Siddha & Herbal Research Centre, Chennai, Tamilnadu, India
Abstract
Fever without an identifiable source in infants younger than three months presents a significant diagnostic and therapeutic challenge due to immature immune responses and subtle clinical signs of serious infection. Although many cases are viral in origin, the risk of serious bacterial infection necessitates careful evaluation. Conventional allopathic management often includes invasive procedures such as lumbar puncture to rule out meningitis. However, parental apprehension toward such procedures may limit their use. This case report describes a 45-day-old infant with persistent fever managed initially under allopathic care with a provisional diagnosis of late-onset sepsis, where lumbar puncture was advised but declined by the parents. Following discharge, the infant was managed using Siddha medicine based on holistic diagnostic principles. The infant showed clinical improvement and resolution of fever without invasive procedures. This report highlights the potential supportive role of Siddha medicine in clinically stable infants with fever without source and emphasizes ethical considerations, parental consent, and integrative clinical decision-making.
Keywords: Fever without source; Infant; Pyrexia of Unknown Origin; Lumbar puncture avoidance; Siddha medicine; Case report
Introduction
Fever, defined as a rectal temperature of ≥38°C (100.4°F), is one of the most common causes of hospital admission in infants. In neonates and young infants below three months of age, fever without a clear source is particularly concerning due to a higher risk of serious bacterial infections such as bacteremia, urinary tract infection, and meningitis. At the same time, infants in this age group may not exhibit focal signs of infection, complicating clinical decision-making.
To minimize the risk of missing invasive bacterial infections, standard allopathic protocols frequently recommend extensive diagnostic evaluations, including blood cultures, inflammatory markers, and lumbar puncture. While lumbar puncture remains a key investigation for suspected meningitis, its diagnostic yield in clinically stable infants without neurological signs is often limited. Moreover, the procedure is invasive, painful, and associated with procedural risks, contributing to parental anxiety and refusal in some cases.
Traditional medical systems such as Siddha conceptualize fever as a manifestation of systemic imbalance rather than an isolated disease entity. Siddha medicine emphasizes restoration of physiological harmony using herbal formulations and individualized assessment. This case report presents the management of fever without source in a 45-day-old infant, focusing on the avoidance of lumbar puncture and the clinical outcome following Siddha therapeutic intervention.
Case Presentation
A 45-day-old infant weighing 4.3 kg was admitted to an allopathic hospital with a history of persistent fever. The infant was breastfed and had no reported seizures, vomiting, respiratory distress, or feeding intolerance at presentation.
Patient Systematic examination and Diagnosis of Allopathy trail
The 45 days of a young baby patient was admitted due to the continuous fever at allopathy hospital. The allopathy practitioner report describes a systematic physical examination of the major body systems— as cardiovascular (CVS) S1: Closure of mitral and tricuspid valves S2: Closure of aortic and pulmonary valves and No murmurs means no abnormal heart sounds were detected. Regarding the respiratory (RS), abdomen (P/A), and central nervous system (CNS)— RS: Bilateral Air Entry Equal. The Soft abdomen means, No guarding, rigidity, or tenderness Non-distended means No abnormal swelling or gas accumulation.
Allopathic Hospital Course
The infant was admitted to the pediatric intensive care unit with a provisional diagnosis of late-onset sepsis. Sepsis screening was performed, and empirical intravenous antibiotics were initiated. A chest X-ray was obtained and found to be normal.
1. Inj. Cefotaxime 200 mg IV every 8 hours
2. Inj. Amikacin 60 mg IV every 24 hours
3. Paracetamol drops (1 ml/100 mg) 0.6 ml every 6 hours
4. Paracetamol suppository 70 mg per rectum (stat dose)
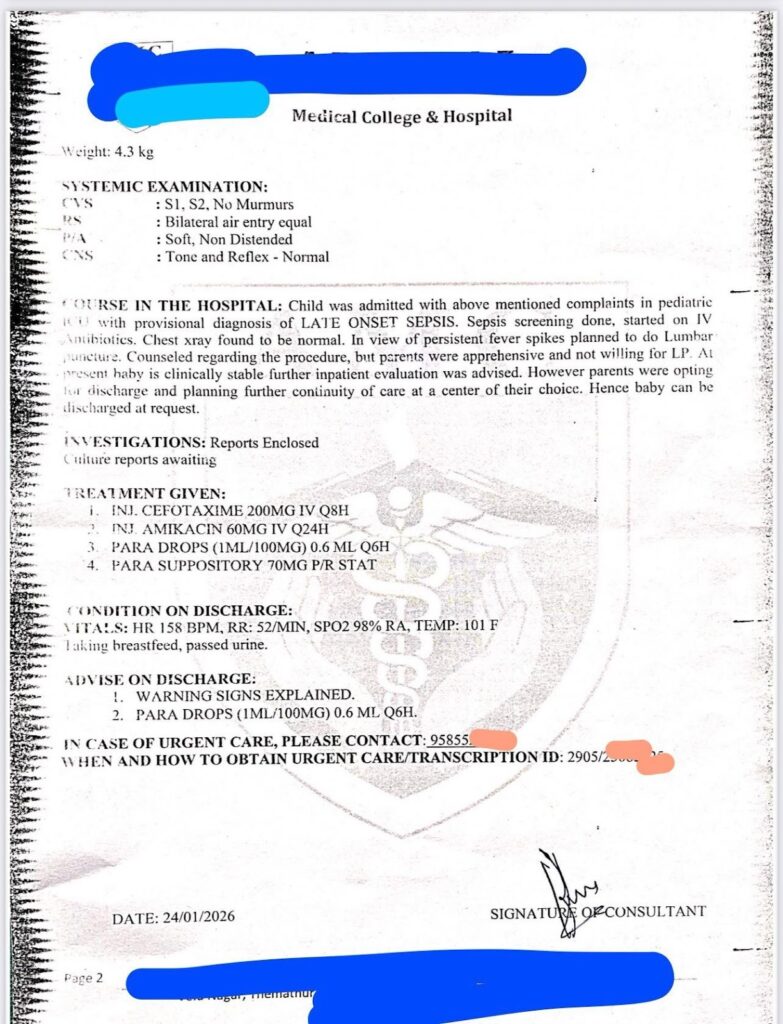
Despite antibiotic therapy, the infant continued to exhibit intermittent fever spikes. In view of persistent fever, lumbar puncture was advised to rule out meningitis. The procedure was explained in detail to the parents; however, they expressed apprehension and declined consent. As the infant remained clinically stable, further inpatient evaluation was recommended, but the parents opted for discharge to continue care at a center of their choice.
Condition on Discharge
- Heart Rate: 158 beats per minute
- Respiratory Rate: 52 breaths per minute
- SpO₂: 98% on room air
- Temperature: 101°F
The infant was not actively breastfeeding and passing urine adequately at the time of discharge. Warning signs were explained to the parents, and antipyretic medication was advised as needed.

Siddha Diagnostic Interpretation
In Siddha medicine, fever is understood as a disturbance of internal physiological balance rather than an isolated pathological entity. Normal body temperature ranges between 36.6°C and 37.2°C (98.6°F), and elevation beyond this range reflects systemic dysregulation. Fever without a definite cause, persisting despite conventional investigations, is clinically comparable to Pyrexia of Unknown Origin (PUO).
Based on the infant’s clinical stability, absence of neurological signs, and normal systemic examination, the condition was interpreted as PUO from a Siddha perspective. The treatment approach focused on restoring equilibrium and supporting innate immunity using herbal formulations.
Siddha Therapeutic Intervention
The infant was administered a Siddha herbal decoction_____ prepared from traditional antipyretic and immunomodulatory herbs. The decoction was given in age-appropriate diluted dosage under careful observation.
Following initiation of Siddha treatment, a gradual reduction in fever spikes was observed. Subsequently, an additional Siddha herbal juice was introduced to stabilize body temperature and support digestion. Over the course of treatment, the infant’s temperature normalized, feeding improved, and no adverse effects were noted.
Vettri herbal juice 200 ml 4 times a day (2+2+2+2)
Herbal juice 100 ml 2 times a day(2+2)
Discussion
Fever without source in infants younger than three months poses a diagnostic dilemma, balancing the need to exclude serious bacterial infection against the risks of invasive procedures. Lumbar puncture, although diagnostically valuable, often yields normal cerebrospinal fluid findings in clinically stable infants and may cause procedural discomfort and parental distress.
In this case, standard allopathic management was appropriately initiated; however, refusal of lumbar puncture necessitated an alternative approach. The Siddha system provided a non-invasive, holistic framework that focused on symptom resolution and systemic balance. The infant’s favorable clinical outcome suggests that, in selected stable cases, traditional medicine may offer a supportive role when invasive procedures are declined.
This case also highlights the importance of ethical practice and shared decision-making in pediatric care. Respecting parental autonomy while ensuring patient safety is crucial, particularly in vulnerable populations such as infants.
Conclusion
This case report demonstrates the successful management of fever without source in a 45-day-old infant through Siddha therapeutic intervention following refusal of lumbar puncture. The infant remained clinically stable, and fever resolved without invasive diagnostic procedures or complications. While this single case cannot establish definitive clinical guidelines, it underscores the potential value of integrative and traditional medical systems in carefully monitored pediatric cases. Further systematic studies are required to validate these observations.

Limitations
This report is limited by its single-case nature, absence of long-term follow-up, and pending microbiological culture results. The findings cannot be generalized and should be interpreted cautiously.
Ethical Considerations
Informed consent was obtained from the infant’s parents prior to Siddha treatment. No invasive procedures were performed without parental approval. Patient confidentiality has been maintained throughout this report.
References
1. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders. Cephalalgia. 2004;24(Suppl 1):9–160.
2. Peskind ER, Riekse R, Quinn JF, et al. Safety and acceptability of the research lumbar puncture. Alzheimer Dis Assoc Disord. 2005;19:220–225.
3. Alcolea D, Martínez-Lage P, Izagirre A, et al. Feasibility of lumbar puncture in cerebrospinal fluid biomarker studies. J Alzheimers Dis. 2014;39:719–726.
4. Zetterberg H, Tullhög K, Hansson O, et al. Low incidence of post-lumbar puncture headache. Eur Neurol. 2010;63:326–330.
5. Blennow K, Wallin A, Häger O. Post-lumbar puncture headache frequency. Acta Neurol Scand. 1993;88:221–223.
6. Laupland KB. Fever in the critically ill medical patient. Crit Care Med. 2009;37(Suppl):S273–S278.